




Australians are living longer, but we’re also living longer with disease and disability. Half of us now have at least one chronic condition.
As rates of disease rise, so does demand for health care. In the 40 years since Medicare began, the average number of visits to the GP per person has increased by more than 60%.
Now general practice – where most people go first for check-ups, diagnoses, and ongoing management of chronic conditions – is under pressure. In 2024, nearly 30% of Australians said they waited too long to get the primary care they needed.
But Australia has more nurses per person than many similar countries. Removing barriers that prevent nurses from using all their skills could help meet the growing demand for care.
Nurses’ skills are being wasted
Primary care works best when delivered by a team: with doctors working alongside nurses, pharmacists, allied health professionals and other health workers.
When the team can safely use all their skills and training, patients benefit from improved access, equal or better health outcomes, improved efficiency and potential cost savings.
However GPs in Australia are less likely than those in similar countries to delegate tasks such as immunisations, routine health checks and health promotion to nurses.
Two recent independent reviews found that while many practices employ a nurse, most are not using all their skills.

Nurses working in primary care agree. A 2024 workforce survey found only one-third of surveyed nurses in general practice regularly work to their full scope of practice.
Nurses are spending too much time doing basic tasks that others could do, taking them away from giving the care they are trained to provide. About 60% of surveyed nurses said they regularly emptied bins or did photocopying.
Meanwhile, less than one-third regularly provided health education and promotion services to patients, despite good evidence that doing so is safe and effective.
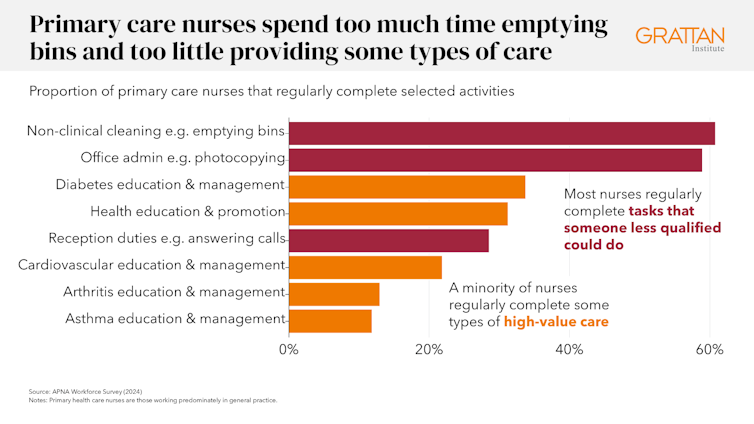
Nurses want to do more. Four in ten said they want to provide health education and promotion services more often.
Nearly half (48%) said they had asked to do more complex clinical activities or extend their role in the past year.
While there is a long way to go, there has been some progress. The proportion of primary care nurses who said they regularly work to their full scope of practice rose from 29% in 2019 to 35% in 2024.
Nurses are being allowed to do more
In the past year and a half, reviews commissioned by the federal government have identified three key areas for reform.
First, the 2024 Scope of Practice Review found confusion across the sector about what nurses can do, and inconsistent rules between states that make it harder for practices to employ their nursing workforce effectively.
It called on federal and state governments to create a national framework that clearly sets out what different health workers can do.
Second, governments and accreditation bodies need to change the way health workers are regulated. Regulation should reflect the activities health workers are trained and qualified to perform safely, not rigid professional boundaries.
State governments should harmonise their legislation – including drugs and poisons acts – so the rules align with workers’ capabilities and are consistent across jurisdictions.
In October, there was a big step forward in expanded and nationally consistent nurse roles. Specially qualified registered nurses will now be able to prescribe medicines.
A funding fix is needed too
Both the Scope of Practice Review and the 2024 Review of General Practice Incentives found changes like these won’t fully succeed without another change: fixing the way Australia funds primary care.
The new rules allowing registered nurse prescribing are one example. Just last week a senate committee unanimously recommended nurse prescriptions should get the same subsidy at the pharmacy as scripts from doctors, instead of costing more as a private script.
Medicare funding needs to keep up too. The current fee-for-service model pays health workers for the number and type of services they provide. This restricts nurse-led care in three ways:
- many services performed by nurses have no Medicare item number
- those that do often have payments that are too low to be viable
- the rules require excessive oversight from a doctor that creates inefficiency.
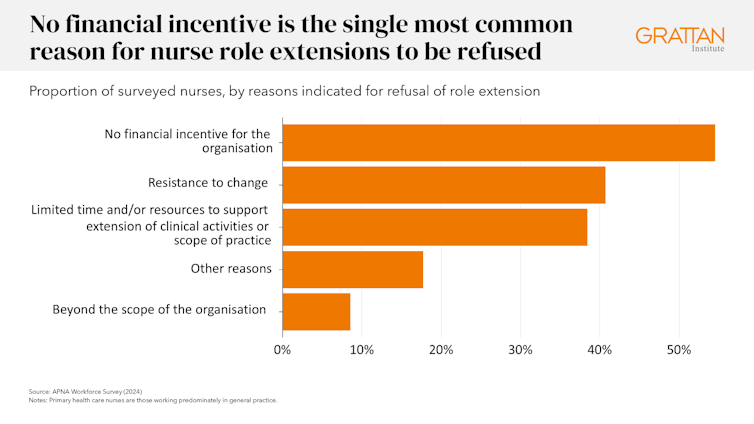
Outdated funding rules are the biggest obstacle to unlocking team-based care. Among surveyed nurses who sought to extend their role and were refused, the single most common reason was a lack of financial incentive for the clinic.
The Scope of Practice Review also found health professionals in fee-for-service settings face the greatest barriers to working to their full scope, while those under more flexible funding models face the fewest.
The solution is a blended funding model
Under blended funding, general practices would receive a lump sum payment to manage a patient’s ongoing care, with higher payments for patients with more complex needs.
This would sit alongside fee-for-service payments for individual consultations and procedures.
More flexible funding would enable clinics to decide how best to deliver care, including when it should be delivered by nurses.
Most countries with similar health systems to ours already use blended funding, and it was backed by both the recent reviews.
Australians’ health needs are getting more complex, and GPs can’t meet them alone. Australia has a large, trusted, and highly skilled nursing workforce. Governments should act now to remove the funding and regulatory barriers holding them back.![]()
Peter Breadon, Program Director, Health and Aged Care, Grattan Institute and Dominic Jones, Research Associate, Grattan Institute
This article is republished from The Conversation under a Creative Commons license. Read the original article.




I am unsure about the general practice receiving a lump sum payment to manage a patient’s ongoing care, with higher payments for patients with more complex needs.
I lived in the UK in the late 1990s and this sounds like the ways GPs were funded then. My opinion was then and still is that it didn’t work. The GP did not refer a patient if they believed the referral was unnecessary, the patient had no say in wanting to see a specialist, the GP decision was the rule.
It was also difficult to see a GP outside the practice you are registered with even if you were away from your home area due to funding concerns. there were times it was hard to be accepted by a practice. I don’t know if that was because my needs were not high enough so the practice didn’t get much money for managing my care. Maybe I am misunderstanding the concept, I hope so.