
I have never been a great advocate for regulated minimum staffing ratios, but prefer regulation of the things that are really important around provision of care services to the people, our care recipients. If you like, having enough of the right people at the right time, and not just to fulfil a compliance requirement around the number of pairs of hands. In completing this Review my own views around staffing, quality of care, industrial considerations and the like have changed – for the better. It remains to be seen if those with the capacity to make an even more profound difference to improve care outcomes for frail, vulnerable, mainly elderly recipients of care – the Australian Government and Parliament – will actually choose to support those whom we serve.
It seems that in Australia rarely a month goes by where the public is not informed of another aged care failing. There is wide spread public perception of a lack of care and low quality of life for residents within the aged care system. The call for greater regulation of minimum staffing standards and additional funds to meet them is prominent but seems to fall on deaf ears of the Australian Government. Without residential aged care provision, residents would likely be inpatients in State based hospitals at several times the daily cost of care of a residential aged care facility. However, the proportion of funds spent on care and service provision should be acquitted on what really matters – the care of people.
This Review discusses the question “If implemented, how will regulated minimum staffing ratios impact on business viability and quality of care in residential aged care services?”
The Review considers:
In aged care in Australia:
In child care in Australia, today 52 per cent of all child care recipients, some 660,000 children predominantly aged four years and below, attend long term day care centres. Child care centres and other children’s services fall under the current National Quality Framework, of which Quality Area 4 of the Framework specifies and regulates for minimum staffing ratios for children receiving child care services. The ‘staffing requirements will vary on the number of places a service is licensed for’.
The following advert appeared in the Weekend Australian of Saturday 12 May 2018.

A direct comparison of residential aged care with child care is difficult. The Aged Care Act 1997 (Cth) (“Act”) provides various forms of legislative and regulatory constraint, accreditation, and practice requirements for service provision. Unlike the child care sector, there is no minimum staffing ratio that protects frail and vulnerable residential aged care recipients. Division 54-1(1)(b) of the Act requires an approved provider ‘to maintain an adequate number of appropriately skilled staff to ensure that the care needs of care recipients are met’. Bowblis comments that in the USA in 1987, nursing homes were required to ‘have sufficient nursing staff to provide nursing and related services to attain and maintain the highest practicable physical, mental, and psychosocial well-being for each resident’. These are surprisingly similar words, likely reflecting a similar structural basis in each jurisdiction.
Pillemer and Moore commented that since ‘the 1960s, patients’ rights advocates have portrayed nursing homes as substandard environments in which patients run the risk of maltreatment’, ‘limitations of patient freedom’, ‘substandard nutrition and living quarters’, and ‘verbal and physical abuse’ as being fundamental problems experienced in nursing home life. Making use of the Maslach Burnout Inventory, Pillemer concluded that nursing home staff are working in highly stressful, complex care environments, where the work is ‘physically very taxing, the wages are poor, and the prestige of the job is low.’ Bowers et al concur adding that, as a strategy, nurses devise ways of ‘keeping up and making up’, and that the emotional care and support of residents and clients is often afforded a lower priority. Wiener, and Shipman and Hooten agree, noting that there is a ‘logical relationship between staffing and quality of care’.
In 2000 the the Queensland Nurses’ Union applied for minimum staffing ratios in residential aged care facilities. Cohen and Spector confirm that ‘higher professional staffing intensity has a positive outcome on resident outcomes. Harrington et al concurred, adding that in the USA a higher minimum standard should be ‘adjusted for resident acuity’. A greater supply and minimum mix of staff seems to be the answer to continuing calls for quality improvement in residential aged care in Australia.
In his review of implementation of staff ratios in California and Victoria, Buchan found that nursing staff ratios are ‘a blunt instrument for achieving employer compliance’. While essentially agreeing, Douglas adds that any solution (to the staffing mix) must ‘strengthen the use of professional nurses; their knowledge, experience, and wisdom are essential’ in care for very frail and vulnerable residents.
Emerging from the literature is the need for a two factor minimum staff ratio. The first is a regulated minimum staff mix that can be a benchmark for all care recipients, and the second is an added component of funding specifically based on the care acuity level of each resident. That acuity level is best described by Park as ‘may be the most important factor in determining both staffing decisions and observed health outcomes’.
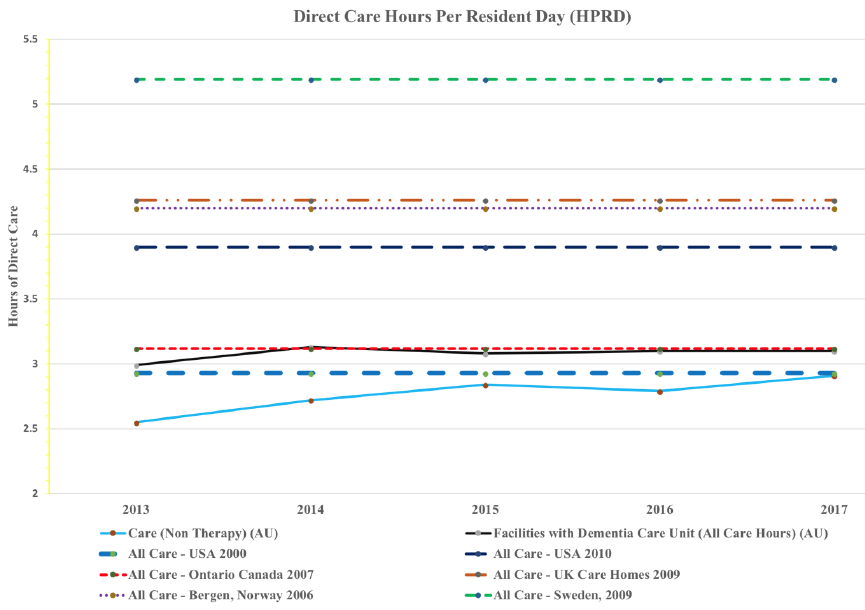
The following chart shows comparable, but only indicative, hours per resident day averaged across all Australian residential aged care, and how it remains well below similar western jurisdictions. The Australian data is sourced from StewartBrown and the international data from Park (USA 2000) and Harrington et al. The summation is that Australia clearly lags behind in its provision of staff resourcing of care for frail and vulnerable care recipients.
Wiener observes that quality of care in aged care facilities remains ‘a major problem for which there is no simple solutions’, and that despite the ‘considerable regulatory apparatus’ the lack of quality may well be a significant reason why so few people would choose to live in them. Admission to a nursing home today is a health-based decision along with the need to receive high quality hospital like care. Wiener adds, ‘increasing staff and raising wages of nursing home workers seem likely to be a necessary precondition to improving quality of care and should be a priority.’ Shipman et al, Hodgkinson et al, Kim et al, Schnelle et al, Lin, and Konetzka et al, all agree, commenting about the evidence of additional registered nurse staff, or additional other nurse and care staff, having a direct positive impact to positively improve the level of quality of care in nursing homes.
Including direct care from registered nurses, enrolled or otherwise certified nurses, and carers howsoever called, and excluding any administrative support nursing and any therapy service hours, on average residential aged care in Australia reaches 2.9 hours per resident day (“HPRD”) as at 31 December 2017. (This only now equates with the minimum benchmark set in the United States of America back in 2000.) The overall cost of residential care services at 30 June 2016 was approximately $11.4 billion for all residential aged care services nation wide If, for example, the minimum staffing ratio of HPRD was raised to 3.2 HPRD, that is, an increase of 0.3 HRPD, and all of this increase was apportioned across the direct care services of registered nurses, enrolled/certified nurses, and carers, on average that will be an approximate increase of ten per cent. That indicates the annual spend on residential aged care increasing by approximately $1.14 billion to $12.54 billion, providing some compensation for the 2016-17 $1.2 billion ‘efficiencies’ reduction. If the increase were to rise to the level recommended by Collier and Harrington27 of 4.1 HRPD, the increase in HRPD is approximately 41 per cent meaning an immediate shortfall in funding of almost $4.72 billion.
In September 2017 the Aged Care Amendment (Ratio of Skilled Staff to Care Recipients) Bill 2017 (“Bill”) was introduced in the Australian Senate. The Bill still sits before the Senate in its Second Reading stage. Whilst not solely focusing on mandated minimum registered nurse ratios, the Bill does suggest that area of primacy. Reflecting on the literature, with the exception of night duty staff, mandating a minimum number of people may be too blunt a manner in which to ensure greater provision of services in any given residential aged care facility. The Bill may be used more as an industrial tool rather than focus on care of residents. However, this review shows the relationship between improved quality outcomes in care is directly related to an increase in both registered nursing staff, and the overall level of care staff.
In terms of law reform, Graycar and Morgan have commented that law reform uses ‘limited consultation processes that often leave out of account the concerns of the most affected. This comment echoes the sensitivity of what providers, clients, and family members alike experience. It is the Australian Government that is leading the change of the aged care sector to a commoditised care market, where people are essentially forgotten, and the balance of equity and justice is outweighed to pragmatic economic models. Of course, cost control is important. The Australian Government currently spends to procure its aged care provision from private providers. It is difficult to conceive that ‘a shift from a focus on person-centred care to organisational profitability’ can always equally apply. Organisations often accommodate progressive funding reductions by trimming their operating budgets, of which workforce is the greatest single cost. The Australian Government should require that organisations demonstrate a level of expenditure on what matters most – care of frail and vulnerable people.
Hutchinson discusses the use of comparative analyses at length within and between jurisdictions, including articles including ‘recommendations for reforming the law informed by the law presented.’ One hopes that the suggestions that follow will be accommodated in the same vein.
This review has considered non-legal matters of importance to the care of frail, vulnerable, recipients of residential aged care services. In so doing, the review suggests that workforce law reform is both obvious and compelling. One wonders where, now understanding what the literature reveals about the significant positive correlation between additional staffing and improvement in quality, if no change is made, the liability for continued poor service quality lies. Many providers would ideally provide additional staff for care, but the accompanying cost impact will drive them to failure. The Australian Government needs to reform the relevant provisions of the quality of care principles in the Act, and allocation the funds necessary to support that change.
This Literature Review has shown that a regulated minimum staffing mix (“Mix”) is an important requirement for residential aged care in Australia. If well planned and implemented, such a Mix is likely to:
i. Have a direct correlation to improved quality of care;
ii. Build the hours of service for all direct care workers;
iii. Include mandatory 24 hours per day, seven days per week, registered nurse cover in all facilities where any one or more resident’s assessed acuity exceeds a certain point on the assessment scale;
iv. Include a minimum of 0.75 HRPD cover by registered nurses;
v. Be based on an immediate increase of HRPD to 3.2 HRPD, with no permissible diminution of current HRPD provision per provider, increasing to 4.1 HRPD over the forward estimates; and
vi. Provide for additional funding from the Australian Government above a minimum benchmark based on the overall acuity assessment per resident.
Further action should commence to amend the relevant legislation reflecting these recommendations, determine the veracity of the initial minimum and phased increase over time, make provision for funding in the forward estimates, and monitor improvements in quality of care and provider agency performance against the implemented minimum standards.








The word staff ratio has been an issue and it is chronic never ending topic and it is sickening.