
The current AN-ACC prescribed care minute allocations, and associated class funding structure, have created an environment of financial favouritism for some residents.
Column B in the table below shows the amount of profit one Lower Means Resident earns by class per day, after prescribed care minute expense is removed from their total funding.
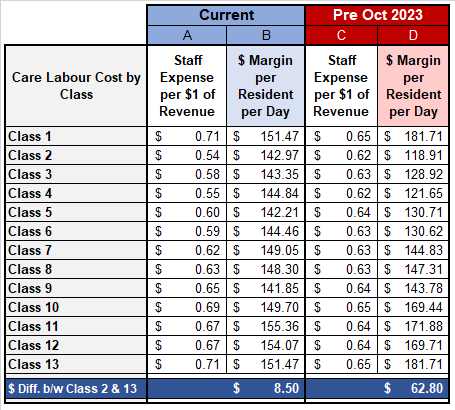
As an example, a Class 2 resident would have a balance of $142.97 remaining from their combined income after total labour expenses have been deducted. This balance is used to fund the non-labour expenses that a provider incurs to meet the needs of the resident.
The variation in margin across classes is slim. The difference between the margins of Class 2 and Class 13 residents is $8.50 per day.
This margin fails to take into consideration the financial complexity of caring for high acuity residents.
Higher acuity residents have substantially greater non-labour expenses. Medical products, continence supplies, allied health, and pharmacy expenses all increase in line with the severity of a resident’s acuity.
Furthermore, due to workload pressure, a wing of high-acuity residents often has significantly greater numbers of staff needing to use their sick leave entitlements.
Ongoing staff absences leads to higher staff turnover and associated costs such as training, casual premiums, overtime, and external agency expenses.
The $8.50 margin between a fully capable Class 2 resident versus a palliative Class 13 resident is insufficient to cover this increased financial burden.
Irregular margins occur across other classes. Residents who are categorised as Class 8 or Class 9 receive the same AN-ACC funding, yet a Class 9 resident has an additional $2,300 of additional labour cost per resident per annum.
These funding anomalies are relatively new. In the Pre-October 2023 funding structure, a Class 2 and Class 13 resident had a margin variance of $62.80.
The unfortunate effect of the unfunded additional costs associated with higher acuity residents means that lower acuity residents are comparatively more profitable. This may discourage care for those that need it most.
In an industry that is as tightly regulated as aged care, there is a moral imperative for financial performance to be subservient to resident care needs. The inconsistencies of the current AN-ACC funding structure are an embodiment of this philosophy.
However, in our industry, there is a balancing act between providing the best possible care while maintaining financial viability. Tip the balance too far in either direction, and success is diminished.
Inadequate funding for high acuity residents places a financial burden on providers, particularly not-for-profits who traditionally have greater expenses, as they run above their prescribed care minute requirements.
A sustainable industry requires all residents, both high and low, Snowballs and Napoleons, to be governed by a fair and consistent funding structure.













